The ultimate shape and configuration of the developing proximal femur are determined by several factors, including differential growth of the bone’s ossification centers, the force of muscle activation and weight bearing, and circulation.
Abnormal growth and development resulting in a misshaped proximal femur is referred to generically as femoral dysplasia (from the Greek dys, ill or bad, + plasia, growth). Trauma or other acquired factors can also affect the shape of the proximal femur. The shape and configuration of the proximal femur have important implications on the congruity and stability of the joint, as well as the stress placed on the joint structures. This topic will be revisited throughout this chapter. Two specific angulations of the proximal femur help define its shape: the angle of inclination and the torsional angle.
Angle of Inclination The angle of inclination of the proximal femur describes the angle within the frontal plane between the femoral neck and the medial side of the femoral shaft (Figure 12-7). At birth this angle measures about 140 to 150 degrees. Primarily because of the loading across the femoral neck during walking, this angle usually reduces to its normal adulthood value of about 125 degrees.16,132 As depicted by the pair of red dots in Figure 12-7, this angle optimizes the alignment of the joint surfaces.
A change in the normal angle of inclination is referred to as either coxa vara or coxa valga. Coxa vara (Latin coxa, hip, + vara, to bend inward) describes an angle of inclination markedly less than 125 degrees; coxa valga (Latin valga, to bend outward) describes an angle of inclination markedly greater than 125 degrees (see Figure 12-7, B and C). These abnormal angles can significantly alter the articulation between the femoral head and the acetabulum, thereby affecting hip biomechanics. Severe malalignment may lead to dislocation or stress-induced degeneration of the joint.
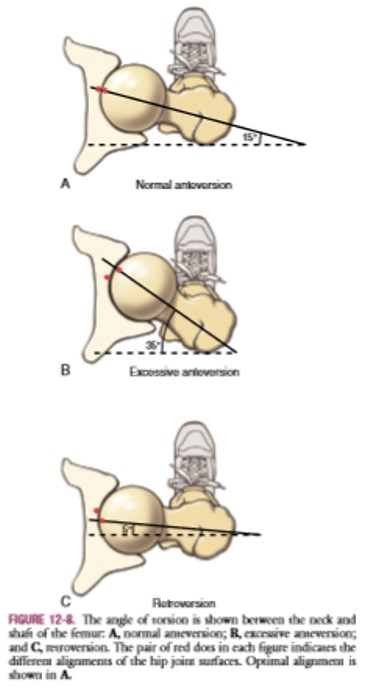
Femoral Torsion Femoral torsion describes the relative rotation (twist) between the bone’s shaft and neck. Normally, as viewed from above, the femoral neck projects about 15 degrees anterior to a medial-lateral axis through the femoral condyles.43 This degree of torsion is called normal anteversion (Figure 12-8, A). In conjunction with the normal angle of inclination, an approximate 15-degree angle of anteversion affords optimal alignment and joint congruence (see alignment of red dots in Figure 12-8, A).
Excessive anteversion in children may be associated with an abnormal gait pattern called “in-toeing.” In-toeing is a walking pattern with exaggerated posturing of hip internal rotation. The amount of in-toeing is generally related to the amount of femoral anteversion. This gait pattern apparently is a compensatory mechanism used to guide the excessively anteverted femoral head more directly into the acetabulum (Figure 12-9). In addition, Arnold and colleagues have shown that the exaggerated internally rotated position during walking serves to increase the moment arm of the important hip abductor muscles—leverage that is substantially reduced with excessive femoral anteversion.9
Regardless of the reason for the internal rotated position, children may, over time, develop shortening of the internal rotator muscles and various ligaments, thereby reducing external rotation range of motion. Fortunately, most children with in-toeing eventually walk normally.163 The gait pattern typically improves with time because of a natural normalization of the anteversion or a combined structural compensation in other parts of the lower extremity, most commonly the tibia.60

There is no evidence that nonoperative treatment can reduce excessive femoral anteversion. Excessive femoral anteversion of 25 to 45 degrees is common in persons with cerebral palsy, and even anteversion as high as 60 to 80 degrees has been reported.8,16 In-toeing typically persists in children with cerebral palsy who are ambulatory and usually does not resolve